Part 1 is mostly about what happened as Bess and I raced against tumor growth to find a new clinical trial that might keep me alive. Part 2 is here, and it is mostly about how this process feels and what could be done differently—and better. If you find this essay useful or interesting, consider the Go Fund Me that’s funding ongoing care.
I thought we were so smart and so well-prepared: Bess and I knew that, if I’m to stay alive, I’d need to swiftly pivot to another clinical trial the moment petosemtamab failed to control the eight squamous cell carcinoma tumors in my neck and lungs. Bess wrote the definitive guide on how to do just that; I’ve written about the extensive work we did between November and January, establishing care at additional hospital systems and even flying out to MD Anderson (MDA) in Houston, to make sure that we’d be ready—just like the French were ready to confront the Germans at the Maginot Line[1] in 1940. In pursuit of that “staying alive” goal, we did so much.[2]
On Mar. 13, we leapt into action, because CT scans showed that the tumors in my neck had grown by 20% since January. We knew that failing to plan is planning to fail, and we’d not made that mistake. Back in November, an oncologist at MDA had been enthusiastic about a Seagen clinical trial of an antibody drug conjugate (ADC) called PDL1V—she cited PDL1V as showing great results in head and neck cancers.[3] Furthermore, Dr. Sacco, my oncologist at UCSD (who dosed me with petosemtamab), had said that UCSD would be getting the Seagen ADC trial in January. Consequently, Bess and I thought we had two good, viable sites for the Seagen trial and felt reassured because of the double coverage. We wouldn’t have to repeat the mad scramble of July and August. We’re pros now, anticipating the pitfalls that made the first search for a trial so trying and so desperate. We also planned for me to get a single dose of chemo to potentially retard tumor growth between trials. We were prepared.
At least, we thought we were prepared.
All of our plans fell apart, and this is the tale of woe of those plans falling apart, and how we tried to maximize the probability of me not dying within a month or two by framing and executing new plans in a fearsome rush against time. Given how fast the cancer has progressed, I may be compromised before a new clinical-trial drug has time to work.
The same week we discovered the petosemtamab had stopped working, we also learned that implementation of the Seagen trial at UCSD had been delayed into mid-April. Unfortunate, we thought, but that’s why we’d readied backup; I messaged MDA in an attempt to get into their Seagen trial. The oncologist I’d met was on vacation, however, and wouldn’t be back until the week of March 25. People go on vacation all the time—wasn’t there someone else I could talk to? I asked if anyone was covering for her, but apparently no one was, and the nurse I corresponded with said I’d have to fly out to see whether MDA might have an appropriate trial, and trial slot.
I was confused, because I’d flown to Houston in November to establish care at MDA to avoid having to scramble in exactly this scenario. Plus, flying is expensive and draining, and I was feeling abysmal. Although I’d been told the previous in-person trip would grant me future remote telemedicine visits, I couldn’t get an appointment. Given how time sensitive cancer can be, saying: “Wait two weeks, and we’ll see” seems not ideal to me. I learned that the MDA phase 1 trial team was considered a different department than the oncologist which I’d seen, and so they (again) wanted me to fly out for basic screening. Maybe the oncologist I’d seen could act as a liaison to find out if the Seagen trial had available slots worth traveling to MDA for, but she was unreachable.
Bess and I have learned not to wait. The healthcare system often moves slowly, and it’s good to be agentic. Insufficient agency is how people die while waiting for some indifferent bureaucrat to get back to them, or for some other bureaucratic process to spin up before the rapidly dividing cancer cells spin someone down.
We began contacting the oncologists we’d met with during the first search. One oncologist warned us that the Seagen trial was so bad that she’d closed it early, because the ADC didn’t work for long and caused so many side effects. What? We were confused. How could we be getting such different views from the oncologist at MDA versus the oncologist whose hospital had closed the trial early?
Nothing made sense. In our efforts to triangulate (quadrangulate? Octa-angulate? We were talking to a lot of people), we eventually met an oncologist at the Fred Hutchinson Cancer Research Center in Seattle (“Fred Hutch”). But when he referenced the NCT for what we thought of as “the Seagen trial” from him, it turned out to be a different trial than PDL1V. That trial was for “SGNTV-001,” not PDL1V! Bess and I thought we were pursuing one Seagen ADC trial when there were (and are) actually two—or really more than two:
* “SGNTV” is Efficacy and Safety Study of Tisotumab Vedotin for Patients With Solid Tumors (innovaTV 207).
* But PDL1V is “A Study of SGN-PDL1V in Advanced Solid Tumors.”
* I’m jumping ahead, but there is at least one other possible Seagen trial, of sigvotatug vedotin (SGN-B6A), that is recruiting and for which I seem to be qualified.
It turns out that saying “I’m looking for the Seagen head and neck cancer ADC trial” is like saying “I’m looking for food.” What sort of food, in what quantity, for how many people, at what cost? We didn’t realize this, and it took us an embarrassingly time to understand it. We weren’t the only ones who were confused. The PIs at various sites didn’t seem to realize that there were multiple Seagen trials, because no one site had more than a single Seagen trial. Since most PIs don’t refer to their trials by NCT, but by the drug company sponsoring the trial, discussing “The Seagen Trial,” meant that both we and the PIs could have what seemed to be a successful conversation about two different Seagen trials. Both trials are ADC trials, making them even more easily confused.
So the oncologist who’d closed the trial early had been talking about SGNTV—Tisotumab Vedotin. Fred Hutch in Seattle had SGNTV slots. UCSD, we found out, was supposed to open an SGNTV site. MDA had PDL1V but not SGNTV. The oncologist at Fred Hutch also said that SGNTV had successfully shrunk a lot of tumors (good), that it had proved durable in some but not a lot of patients (not as good), and that the side effect profile was pretty bad, with a fair number of patients having to exit the trial because of ocular side effects in particular.
Moreover, both SGNTV and PDL1V have peculiar rules that exclude a lot of patients from clinical trials: patients can have at most two previous systemic lines of therapy in the recurrent/metastatic setting. Last summer and early fall, I received pembrolizumab (Keytruda) and two cycles of chemotherapy, which consisted of carboplatin and paclitaxel. Then I got petosemtamab. The pembro and chemo were received at the same time, and can, if looked at properly, be considered part of the same line of therapy. If I was given SGNTV, I’d have three systemic lines of therapy and be ineligible for PDL1V. And the same in reverse. Sophie’s Choice!
Still, the oncologist at Fred Hutch said that I’m eligible for SGNTV, he had a slot for SGNTV, and he thought SGNTV a reasonable choice. Without knowing whether I might be able to get a PDL1V slot at MDA, or somewhere else, Bess and I debated and elected to go ahead and do SGNTV, risking the ocular and other side effects. But then we heard back from him the next day: “You’re over the limit on lines of therapy.” But the rules on clinicaltrials.gov said “no more than 2,” which is exactly what I’d had. That confused us, so we asked for more detail, and he replied that SGNTV “will not allow more than 1 line of treatment in the metastatic setting, that is why you are not eligible, its independent of how we count the chemo.” Huh? I’d read the clinicaltrials.gov requirements.
Much later, we learned from Dr. Sacco that there are rules upon rules: different “arms” of the SGNTV trial have different eligibility criteria. I was eligible for Arm C, I think, but not most of the other arms. Still, we were interested to see if anyone else interpreted the rules differently, which, as we learned during the first search back in July, happens routinely. We sought SGNTV at sites in Oregon and Stanford. One said the SGNTV is closed, and the other said I’m not eligible due to limits on prior lines of therapy, confirming that updates to the rules don’t have to be updated on ClinicalTrials.gov. Around the same time, someone helped us to learn that the UCSD trial would either not open or not open in time for it to be relevant for me.
So we gave up on SGNTV and wheeled around to seek PDL1V.[4] You may recall that I mentioned wanting to get a single dose of chemo in as a bridge between trials, to prevent the tumors from ballooning or killing me. I didn’t get that chemo dose immediately, however, because a lot of drug companies are bizarrely finicky about things like interpreting the meaning of lines of therapy, and I didn’t want to inadvertently render myself ineligible for good trials. If you’re already exhausted by the barrage of issues and considerations, don’t be discouraged: you’re not alone. I’m exhausted by this process, and for me the wrong answer is fatal. I’ve barely written between Mar. 18 and now because the clinical-trial process, combined with increasing fatigue and pain, have occupied almost all of my time, attention, and energy. I’ve done tiny amounts of Twitter between phone calls and research bouts, but I’ve not managed anything substantive because of my focus being stolen. Bess has been similarly quiet, for similar reasons, and because she’s begun working full-time in the emergency room again.
Anyway, to return to the PDL1V issue, two of the more proximate sites were available under the same umbrella organization, the START Center for Cancer Care: one site in San Antonio, the other in Salt Lake City.[5] Both START sites were incredibly responsive: both nearly immediately confirmed that they would host PDL1V, pre-screened me for eligibility, and started the paperwork process (“the paperwork process” is frustrating but universal, in our experience so far). Neither START site would make me fly out before the required in-person consent. I wouldn’t have to travel until they’d officially reserved and confirmed a spot; START said that making patients fly out just for screening is unnecessarily cruel to patients who are already overwhelmed and suffering: a kindness that did not go unnoticed. We were told that the new arm of PDL1V—the “c” arm—would likely be open in mid-April. I think we learned that sometime in the Mar. 20 – 26 timeframe, but I don’t have the energy now to search through dozens of notes and hundreds of disparate emails for answers that aren’t of fundamental importance to the story.
While this was going on—I’m telling the story somewhat out of order, because maintaining the precise order would make it even more exhaustingly minute than it already is—we were also making appointments with some of the other oncologists and hospital systems. A surprising one is Hackensack Hospital, which is part of Meridian Health. If you have head and neck cancer and live in the northeast, it turns out that there are three essential hospital systems. Two are obvious: Memorial-Sloan Kettering (MSK) in New York City and Dana Farber in Boston, and our experiences with both have been fantastic (not because there is less bureaucracy, but because the doctors we dealt with there were not completely beholden to it). The third is Hackensack, whose quality appears to rest primarily on the capabilities of Dr. Gutierrez, who is invested in choosing a few, but quality, trials, accepts initial telemedicine visits, and seems to understand that speed matters in rapidly progressing diseases. I’d not have guessed Hackensack Hospital would be a great place for head and neck cancer clinical trials, and I would’ve been wrong. From Dr. Gutierrez at Hackensack, we learned about an immunotherapy trial called BGB-A3055 (I didn’t invent the naming nomenclature). BGB-A3055 has no lines-of-treatment restrictions and an arm of it that includes tislelizumab (another pembro-like antibody) is supposed to open in April.
So BGB-A3055 was another possibility, although I think it just recently entered phase 1b and there’s little or no published data on it. Around the time we were learning about BGB-A3055 from Dr. Gutierrez, we also met an oncologist named Dr. Weight at Sarah Cannon in Denver. Dr. Weight told us about a trial for ABBV-400, another ADC that uses a different mechanism than PDL1V, and said that it has also shown some success in some head and neck patients. A downside of all these phase 1b studies is that there’s little published data, which makes comparisons difficult. Oncologists almost never give numbers: “We dosed 10 patients, and the disease control rate in phase 1a was 50%.” Instead, they’ll be vague, but they’ll also indicate why they think their top trials are their top trials. Strangely—or perhaps not strangely—we found more preliminary data was provided to investors by the drug companies in investor reports, than was given to oncologists or patients. We shared slides from investor pitches with oncologists, who were also surprised to see even early spider graphs of data that hadn’t crossed their desk.[6]
Bess and I spent a lot of time debating the sometimes gnomic descriptions of various trials—it’s like listening to people talk about wines: is “oaky” good while “tannic” is bad? “Mineral forward” versus “fruit notes?” I have no idea. We had to decide between oncologists who have seen “some responses” in head and neck, versus the ones who have seen “good responses.” Or the others who have seen “some activity.”
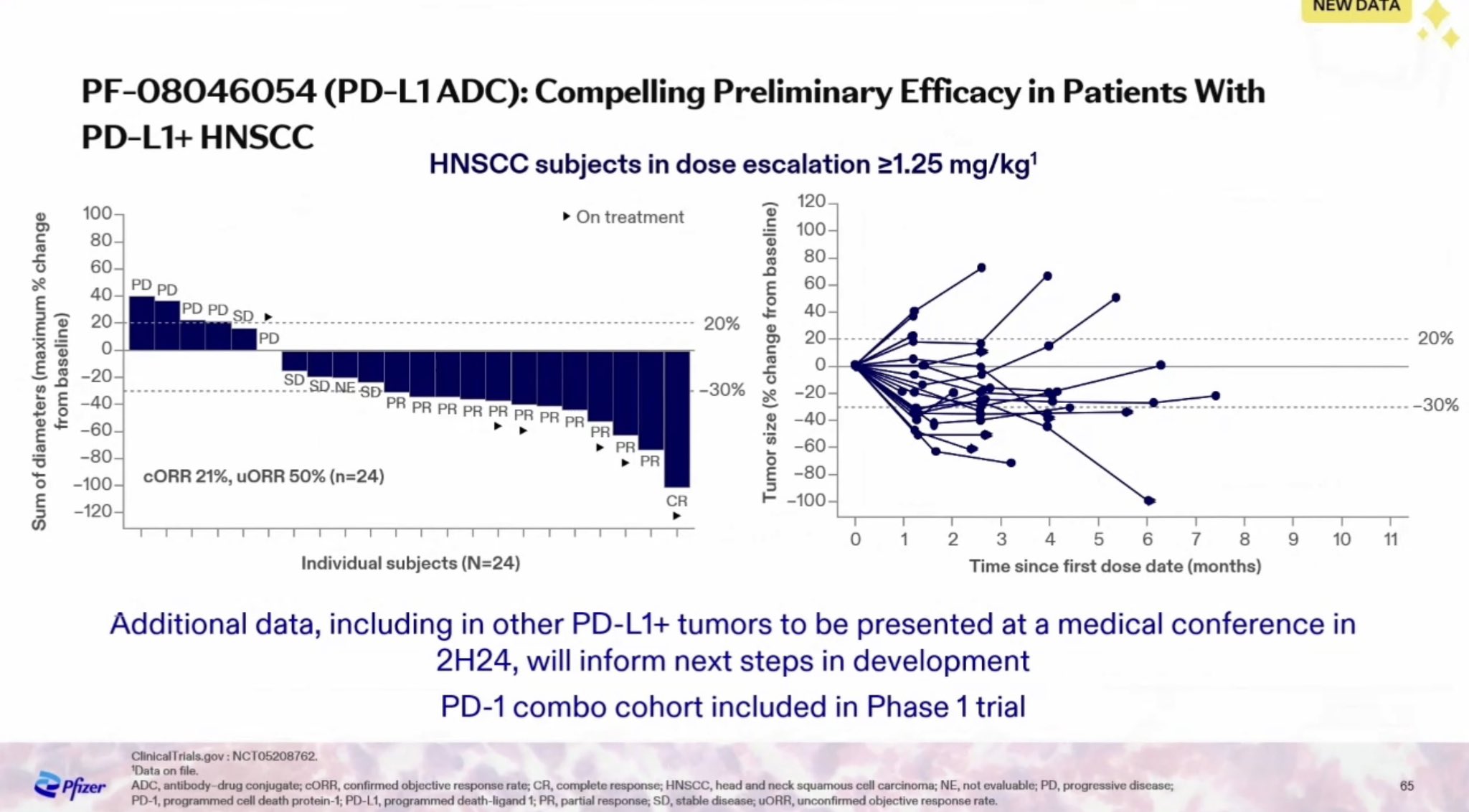
We also had to figure out what might available. BGB-3055 would open in April—around the same time as PDL1V. There was also a site called NEXT in Dallas that was offering the trial. ABBV-400 was immediately available, which was attractive. I found a single slide from a Feb. 29 Pfizer presentation to investors, via a Google search that brought me to a biotech investor’s tweet:
While this was going on, we kept trying to get MDA’s phase 1 clinical trials department to recommend some trials to us, but they wouldn’t. Bess faxed all my information to MDA (healthcare systems use the world’s fax machines and pagers, stuck as they are in the past), with pleas for a return e-mail or phone call, but none came. She also tried leaving messages with the department, and cold e-mailing PIs. No luck. We’ve learned that if someone won’t, or can’t, spend the cash and energy to show up in person, MDA isn’t the right place. This is surprising to me, given how hard flying is for many cancer patients, how expensive cancer is, and given the fact that we’re not living in 1995 and have digital records, but at some point the organization behaves how it behaves and the culture is what it is. We did get some unexpected help from someone at MDA (thank you! you know who you are), who tried to facilitate conversations between us and the right departments, but even that person couldn’t break through the bureaucracy. By the time we finally heard back from the oncologist at MDA, START was already moving me along the qualification process for PDL1V. Plus, the MDA oncologist said I wasn’t eligible for PDL1V. Bess and I were baffled, and might have asked why she thought I wasn’t eligible, but she’d turned off the “reply” feature in MDA’s EHR; it didn’t seem worth starting a new message thread. I was already tracked to start at START.
We decided to focus on PDL1V, the main reason being that, if I got another trial, I’d lose it forever due to the lines-of-therapy limitation; BGB-3055 and ABBV-400 don’t have lines-of-therapy limitations. Secondarily, that Pfizer slide shows three-quarters of patients responding to it, which is good by HNSCC standards. Somewhere in this ordeal, we also asked START if I could do a round of chemo and still qualify for PDL1V. START-San Antonio initially thought the answer was yes: getting a round of the exact same chemo I’d had in summer 2023 should be fine. We made appointments.
START-Utah thought the same based on what was written in their provider guidelines (we’ve learned to double check whenever possible). But Pfizer had scheduled a meeting later in the week to discuss updated guidelines, which mean the guidelines might be different in four days, and the answer obsolete. Bess asked if they could confirm with Seagen’s “medical liaison,” who makes the final eligibility decisions. The tumors in my neck were visibly growing, so I was worried about whether I’d make it to mid-April, and even a delay of a few days could affect my “washout period” and the timing when I could start the trial. But I delayed while waiting for their answer. Pfizer’s decision: Any more chemo will count as a new line of therapy. If we hadn’t known to ask about the meeting, to ask for the medical liaison, to clarify and clarify again, I’d have lost a potential spot. We shelved the plan to get chemo.
In slightly good news, we were told that, if a patient fails the previous line of therapy, there is only a two-week washout period. So I could at least get one more round of petosemtamab, on the off chance that I wasn’t entirely resistant, which Dr. Sacco agreed to arrange. I flew back to San Diego on Mar. 28 for an infusion on Mar. 29. Did that infusion do anything? Probably not, but maybe, and it was something. Bess and I were watching the tumors in my neck grow larger seemingly by the day. At least the petosemtamab had kept the tumors in my lungs more or less in check.
Dr. Sacco also said that many trials will let patients get some spot radiation in an attempt to shrink tumors enough for the patient (me) to survive. We contacted Dr. Patel at Mayo Phoenix about this, and he was like: “Makes sense! Let’s do it.” We told him about the back-and-forth regarding whether I’d actually be eligible, and he’s clearly seen this game played before, because attitude was: “Let’s schedule a simulation so that you can get your mask made and be ready.” Beautiful. And easy! I got the radiation simulation Apr. 4
START told us that Pfizer was holding a kickoff meeting the first week of April. That meeting happened, and we planned to target START-Utah, since Utah is closer to Arizona than San Antonio. There was some kind of unspecific institutional review board (IRB) holdup as well. Ultimately, START said that I could get consented on Apr. 8, so I got a last-minute (meaning: $$$) ticket to Utah for Apr. 7. Unfortunately, START doesn’t have its own CT machine on site, so getting the mandatory CT scans became yet another logistical challenge; I will spare the details, apart from saying that something as simple as getting CT scans locally couldn’t go smoothly, resulting in a seven-hour day to get 60 seconds’ worth of scans, an experience that might seem minor in the grand scheme of suffering, but which showcases the accumulation of seemingly minor problems that together become crushing. It was exhausting. I was exhausted. I am exhausted. You are probably exhausted just reading this.
I was so exhausted that I considered whether I wanted to terminate treatment, or just do local phase 1a trials, which is nearly equivalent to terminating treatment, because 1a dose-finding trials start with such low concentrations of active medicine that, even if the medication ultimately works, the initial people who get it probably won’t see a response. I was sick. I was tired. I was sick and tired of fighting bureaucracy. Bess and I spent a month continuously wrangling an inefficient, balky medical system. The void felt better than continuing the fight—not the fight against cancer, but the fight against the balkanized clinical-trial system.
Ultimately, I went through with the PDL1V trial, flying to Utah on Apr. 14 and receiving the first dose on Apr. 15. The worst parts of the process were behind me. It’s saying something when the “worst part” isn’t the actual infusion of a largely untested study drug. It isn’t even the fatigue that followed. But I want to spend as much time with Bess as I can, before the curtain falls, as it will likely will soon enough. I worry that I’ll get hit with a pulmonary embolism (PE), stroke, cardiac event, sudden breach of critical blood vessels by tumors—and I’ll feel a sudden pain in my head or neck, then nothing. PDL1V could delay that moment.
In “The Council of Elrond” from The Fellowship of the Ring, Gandalf gives an account of his captivity by the traitorous Saruman, and he says: “May Elrond and the others forgive the length of it.” May you forgive the length of this account.[7] It gives a flavor of my life, but it may also prove educational to patients who are suffering as I have—firstly from cancer and other dread diseases, but secondly from the process of searching for treatment.
Part 2 is here. If you’ve gotten this far, consider the Go Fund Me that’s funding ongoing care.
[1] “Ligne Maginot” in French, according to Wikipedia.
[2] In my case, cancer also chose to take the Belgian route, bypassing our defenses and leading to my personal Dunkirk, except even more disastrous.
[3] ADCs are hot in oncology because results so far show them as being efficacious and with fewer side effects than things like chemotherapy. One description says ADCs “couple two therapies, basically work like guided missiles. A toxic warhead is strapped to a missile that homes in on and drops its payload on a specific tumor.” PDL1V contains a chemo agent called MMAE, which Wikipedia says shows “potency of up to 200 times that of vinblastine.” Seagen is a, or the, leader in ADCs, and Pfizer just bought it for $43 billion, which is a vote for ADCs’ potential.
[4] We were also interested in a small-molecule called NT219, but that drug had completed its phase 1b trial and hasn’t yet moved to phase 2 or approval—so another promising candidate from our previous research was lost to us.
[5] Dr. Sacco also recommended an ADC trial, if possible, because of the amount of research (and money) are indications that that mechanism of action is likely to work.
[6] One reader suggests: “The Hippocratic oath may be incompatible with capitalism if shareholders continue to be prioritized over the researchers who desperately need this data in order to make informed decisions for patients like me.” My view is different: the FDA rules that drive and create this insane process are imposed by government. The drug companies want to sell drugs! I want to take drugs. For fatal diseases like R / M HNSCC, there should be basic safety studies—essentially phase 1a and 1b studies—and from there oncologists should be allowed to prescribe novel therapies.
[7] Gandalf’s captivity is not just physical but also involves psychological dimensions as he deals with isolation, uncertainty, and deception. Cancer patients face emotional and mental torment, dealing not only with their physical illness but also with the psychological burden of managing their treatment process, which is often opaque—and, in my case, unending, or rather ending only in death. Most of the clinical trials see a tiny number of patients get “complete response,” or the apparent elimination of their cancers, but that is so rare that I’m discounting it for myself.


This might sound silly, but is there any sort of Yelp type platform that tracks and surfaces the reputational quality of these cancer centers? When “regular” businesses become bureaucratically or technologically outdated, they usually face market pressures to either adapt or begin to lose revenue. Is there any market mechanism that “punishes” an institution like MDA for being so rigid?
LikeLike
You are a courageous man. More so for sharing your journey publicly.
In matters of health, I’ve come to realize a single truth over my lifetime – what’s best is what works. And what works does so for a reason.
The current state of modern allopathic medicine forged by alliances between three letter agencies, pharmaceutical industries, and medical institutions chasing grant dollars don’t always support what’s best and what works.
There are no coincidences in life. I’m some random guy that’s stumbled onto your blog post and I will leave you with this.
May you heal with whatever works for you. I wish you well.
https://open.substack.com/pub/veryvirology/p/curing-the-incurable-cancer
LikeLike